

Background: Pyruvate kinase (PK) deficiency is a rare, inherited disorder caused by autosomal recessive mutations in the PKLR gene, whereby a glycolytic defect causes reduced adenosine triphosphate levels and leads to hemolytic anemia. Patients with PK deficiency can experience serious complications associated with the disease and its treatment, including osteoporosis, pulmonary hypertension, sepsis, iron overload, and liver cirrhosis. The current standard of care for PK deficiency is supportive, including blood transfusions, splenectomy, iron chelation therapy and/or interventions for other disease-related morbidity. There is no approved therapy for this condition. Identifying PK deficiency in real-world data is challenging due to a lack of diagnosis codes and treatments that are specific to PK deficiency. As a result, population-based studies of PK deficiency using claims or electronic health record databases are limited. In addition, data on mortality in this patient population are lacking and limited to a few individual case reports. This study aimed to identify patients with a PK deficiency diagnosis as documented by physicians and to compare their mortality to an age- and gender-matched cohort of individuals without PK deficiency.
Methods: Patients with ≥ 1 diagnosis code related to PK deficiency (i.e., anemia due to disorders of glycolytic enzymes [International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) D55.2], other hemolytic anemias due to enzyme deficiency [ICD-9-CM 282.3], or unspecified hereditary hemolytic anemia [ICD-9-CM 282.9, ICD-10-CM D58.9]) between January 1995 and July 2019 were selected from the US Veterans Health Administration (VHA) database. To be considered for inclusion, physicians' notes were required to contain the words "pyruvate", "kinase", and "deficiency." A manual review of these physicians' notes was performed to identify patients with a physician-documented diagnosis of PK deficiency (PK deficiency cohort). The index date for the PK deficiency cohort was defined as the date of the first medical record with a diagnosis code related to PK deficiency. Each patient in the PK deficiency cohort was matched 1:5 by age at index, sex, and index year (± 1 year) to patients from the general VHA population with no diagnosis codes related to PK deficiency (non-PK deficiency cohort). The index date for the non-PK deficiency cohort was defined as a random visit date during their match's index year. Survival time from the index date was compared between the PK deficiency cohort and their non-PK deficiency cohort matches using a univariate Cox proportional hazards model with robust standard error estimation.
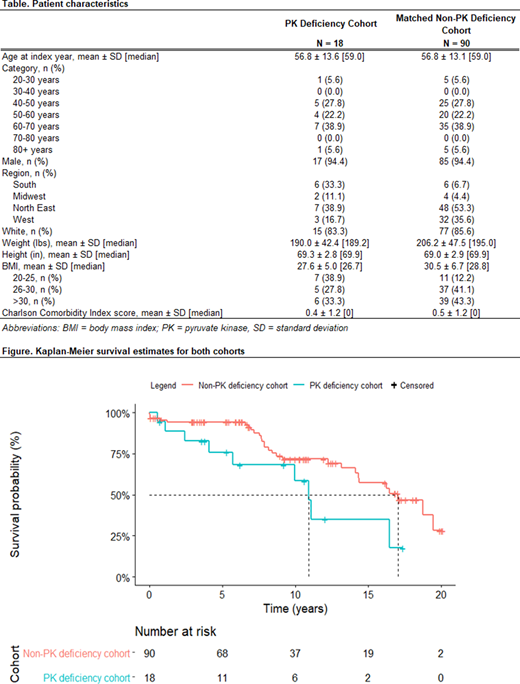
Results: A total of 18 patients met inclusion criteria for the PK deficiency cohort and were matched to 90 individuals in the non-PK deficiency cohort. Baseline characteristics for both cohorts are shown in the Table. For both cohorts, the mean age at index was 57 years and 94% of patients were male; 83-85% were white and the mean Charlson Comorbidity Index score was 0.4-0.5 (no significant differences between cohorts). Imbalances remained between the two cohorts with regard to region and body mass index.
The median follow-up was 6.0 years for the PK deficiency cohort and 8.0 years for the non-PK deficiency cohort. Over the follow-up period, there were 9 (50%) observed deaths in the PK deficiency cohort and 28 (31%) observed deaths in the non-PK deficiency cohort. The median time until death was 10.9 years for the PK deficiency cohort and 17.1 years for the non-PK deficiency cohort; the Kaplan-Meier curves for both cohorts are shown in the Figure. Patients in the non-PK deficiency cohort had a significantly longer time to death than the PK deficiency cohort (hazard ratio: 2.3; p = 0.0306); 10 years after index, 42% of patients in the PK deficiency cohort had died compared with 28% of those in the non-PK deficiency cohort.
Conclusions: The results of this study suggest that patients with PK deficiency may be at an increased risk of mortality. Further research to understand cause of death in this population is warranted, as is the replication of this study using larger sample sizes and other real-world data sources that better represent females and the pediatric and adolescent PK deficiency age groups.
Zagadailov:Agios Pharmaceuticals: Current Employment, Current equity holder in publicly-traded company. Boscoe:Agios Pharmaceuticals: Current Employment, Current equity holder in private company. Garcia-Horton:Agios Pharmaceuticals: Consultancy; Analysis Group, Inc.: Current Employment. Shi:Agios Pharmaceuticals: Consultancy; Analysis Group, Inc.: Current Employment. Liu:Analysis Group, Inc.: Consultancy. Shi:Analysis Group, Inc.: Consultancy. Macaulay:Agios Pharmaceuticals: Consultancy; Analysis Group, Inc.: Current Employment.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal